Mechanical vs Neurogenic Limitations in Ocular Motility
Welcome to Bitesized Orthoptics! Your go-to series for quick, focused refreshers on key orthoptic topics.
Whether you're prepping for exams, on your way to clinic, or revising a tricky concept, these short reads break down core ideas into digestible pieces. No fluff. No overwhelm. Just clear, concise overviews to boost your confidence and clinical understanding — one bite at a time.
Understanding whether an ocular motility restriction is mechanical or neurogenic is one of the most important clinical distinctions in orthoptics. Although both can present with restricted eye movements, the underlying mechanisms and their clinical patterns can be very different. A systematic approach allows orthoptists to confidently differentiate between the two.
Forced Duction Test (FDT)
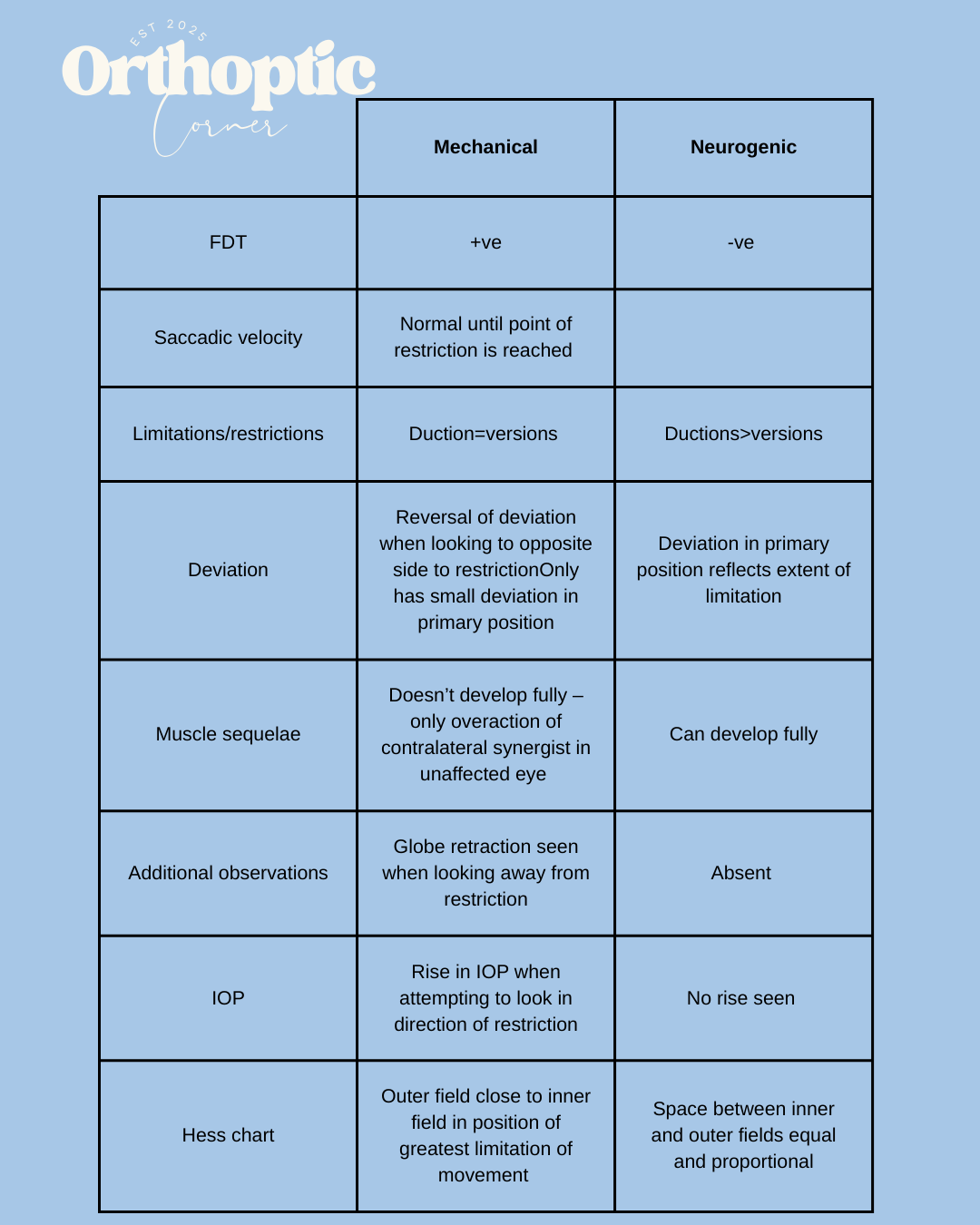
The FDT remains one of the most definitive tools for distinguishing mechanical from neurogenic causes.
Mechanical: The test is positive. Resistance is felt when moving the globe into the restricted field, confirming a physical or structural block such as a tight tendon, entrapment, fibrosis, or adhesions.
Neurogenic: The test is negative. There is no mechanical resistance, and the globe moves fully when passively guided—despite an active motility deficit. This reflects muscle weakness or impaired innervation rather than a structural limitation.
Saccadic Velocity
Saccadic assessment is a useful functional marker.
Mechanical: Saccades are normal up until the point of restriction, at which movement abruptly stops. The early part of the saccade looks healthy because the muscle itself is not weak, movement is simply blocked
Neurogenic: Saccades are slow and hypometric throughout the entire movement range. This is classic for paretic or underacting muscles.
Ductions and Versions
Comparing ductions and versions helps reveal the nature of the limitation.
Mechanical: Ductions and versions are roughly equal because the restriction is present regardless of binocular or monocular viewing.
Neurogenic: Ductions are greater than versions. When the affected eye is fixating, its movement is limited, but when the fellow eye fixates, the affected eye may move further due to Hering’s law and increased innervation.
Deviation Patterns
How the deviation behaves across gaze positions will provide you with clues:
Mechanical:
There is often reversal of the deviation when the patient looks to the opposite side of the restriction.
Deviation in primary position is usually small, as the restriction may not significantly affect primary alignment.
Neurogenic:
The size of the primary position deviation often reflects the degree of muscle weakness
No characteristic reversal pattern is seen. The deviation increases in the field of action of the weak muscle.
Muscle Sequelae
Mechanical: Sequelae do not fully develop. Only an overaction of the contralateral synergist may appear, and even this is often mild. The classic cascade of underaction/overaction that we see in neurogenic palsies is typically absent.
Neurogenic: Full muscle sequelae develop according to the pattern of primary underaction with secondary overaction of the ipsilateral antagonist and contralateral synergist.
Additional Clinical Observations
Small structural or movement cues often reinforce the diagnosis.
Mechanical: Globe retraction may be seen when the patient looks away from the restricted field. This can occur due to tight tissues physically drawing the globe backward.
Neurogenic: Retraction is absent because there is no mechanical tethering.
Intraocular Pressure (IOP)
Tonometry in different gaze positions is an underutilised but powerful diagnostic tool.
Mechanical: Attempting to look into the restricted field causes a measurable rise in IOP because the globe is pushing against a mechanical barrier.
Neurogenic: No significant rise is seen since no physical restriction is present.
Hess Chart Findings
Mechanical:
The outer field lies close to the inner field in the direction of maximum restriction.
This reflects equal limitation of monocular and binocular movement.
Neurogenic:
The spacing between inner and outer fields remains equal and proportional, reflecting a consistent neurological deficit rather than a mechanical block.
Summary: